A Blind Man Sees with Technology . . . and Practice
By Lydia Denworth | May 22, 2014 | Psychology Today | Topics: Learning, Science and Health
How brain training might help recipients of retinal implants

Roger Pontz working with low vision therapist Ashley Howson as his wife, Terri, looks on
At the age of fourteen, Roger Pontz was diagnosed with a degenerative condition called retinitis pigmentosa. For the next forty years, his eyesight grew progressively worse until he was completely blind in his early forties.
But he’s not anymore.
In January, Pontz, now 55, became the second American to receive a retinal implant after the devices became commercially available this year. Developed by Second Sight, a California company, and approved by the FDA in 2013 only for adults with retinitis pigmentosa, the Argus II prosthesis uses a camera on a pair of glasses to send a wireless signal to the retina, where surgically-placed electrodes send the information to visual areas of the brain. “Patients receive spots of light just like the lights on a scoreboard or the pixels on a computer,” says Robert Greenberg, President and CEO of Second Sight. “It’s much like a crude black and white television.”
Pontz, of Reed City, Michigan, had hoped to be part of the clinical trials, but didn’t live close enough. He was thrilled when retinal surgeon Thiran Jayasundera at the University of Michigan Kellogg Eye Center in Ann Arbor became the first to perform the commercial implants.
By waiting, Pontz got an unexpected benefit: rehabilitation. Unlike in the trials, every commercial implant recipient—the fifth surgery in the United States is scheduled for this week, and more than fifty have been done in Europe—receives a rehabilitation kit and low vision therapy (the duration and intensity of the therapy varies.) Pontz visits the clinic once a week and practices with his wife, Terri, daily. “Every day I’m picking up something new,” he says.
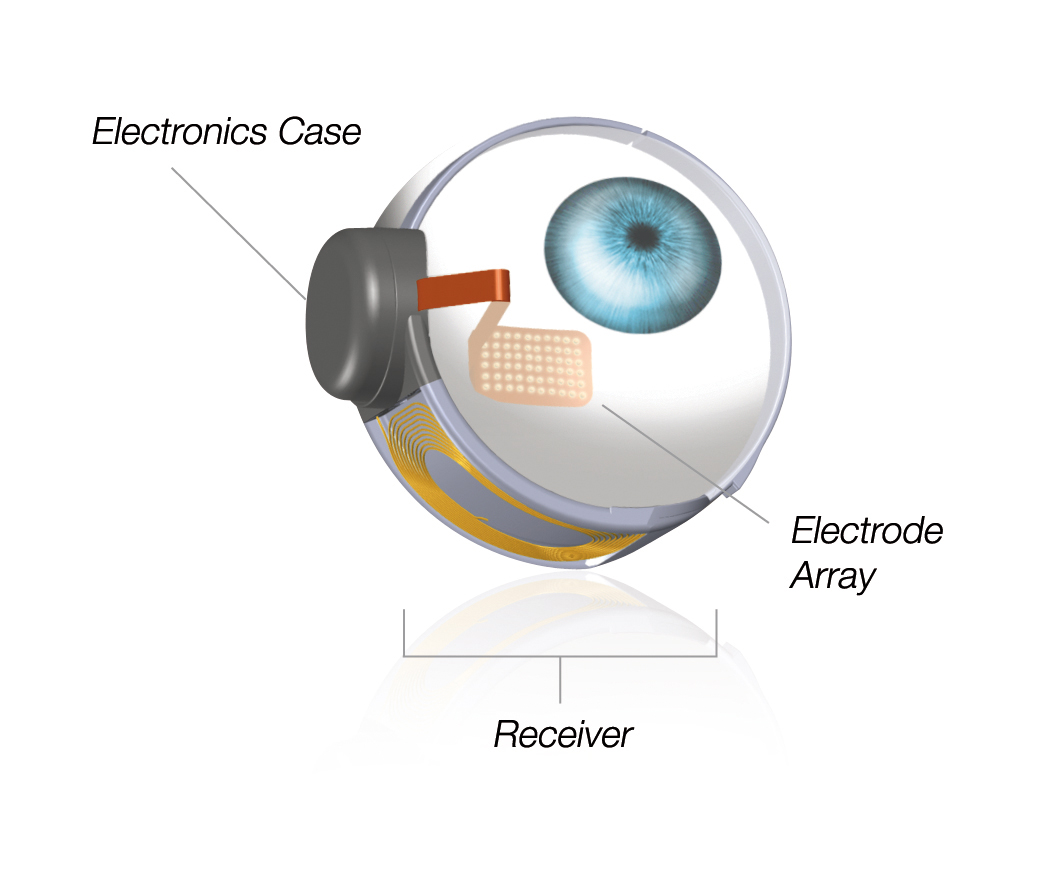
The Argus II
Like high contrast toys for babies, the kit includes black and white pieces of felt, and a white easel board with a set of black magnetic shapes. First, Pontz had to distinguish the black felt from the white. Then he had to locate white plates on dark tablecloths and vice versa. “The other day Terri had a bowl and asked if I could see it,” says Pontz. “I went, yeah, right there! And I bumped my two fingers in her oatmeal!” He laughs. “I try not to hesitate. I just reach out and grab it.” The next challenge is identifying four-inch circles or squares on the easel.
Training to use an implanted device seems an obvious idea, given the brain’s capacity to change with experience. With retinal implants, Greenberg admits, it was an after thought. “Just getting the technology to work was such a major focus,” he says, “that it wasn’t until we worked out some of the bugs with the surgery and the device that we were able to turn our attention to asking: How can we improve the utility to the patients?”
Brain plasticity wasn’t initially thought to be an important factor since retinal implant patients must be adults. The greatest periods of brain development come in childhood, when the brain is generating new neurons, strengthening connections between those that are used regularly, and pruning those that are not. “The general feeling was that adults didn’t have the plasticity,” Greenberg says, “or the time [for therapy].” Even with cochlear implants, which have been around for decades, children routinely receive therapy to help them hear with the device, but adults do not.
In restoring some vision with the Argus II, mobility and orientation were the main goals, but the best patients read large letters. “It seemed like there was a natural learning curve where patients got better and better at using the device over the first year,” says Greenberg. Prodded by low vision therapists, his team wondered if providing tools and explicit help could speed that learning curve and perhaps help patients achieve even more than they otherwise would.
According to the American Academy of Ophthalmology, there’s a new awareness of the possibilities of low vision rehabilitation for patients of all sorts. Some of the therapy simply concerns learning coping strategies. But it’s also believed that even in adulthood, visual brain networks can be strengthened with effort and repetition. Doctors have been pleasantly surprised by the adaptations even older patients can make.
Second Sight doesn’t have hard data yet to show that the rehabilitation is helping retinal implant patients, but they’re taking the view that extra practice can’t hurt.
Pontz, who works as a dishwasher in a bowling alley, believes his hard work is paying off. “The more you use it, the more you adjust to it,” he says. “I used to have to put my hands out in front of me when walking through the house and I’d run into things a lot. I don’t do that anymore.” He can tell if his wife is wearing light or dark clothing and he can grab the handle on the refrigerator. “If this is all I gained out of it, I’d be happy,” he says. “But I see me gaining a lot more.”
He’d like to be able to see the pins at the end of the bowling alley. He’d like to be able to play basketball with his grandson. Most of all, says Pontz, “I’d like to see my wife.” Maybe, with practice, he will.